This article has been expanded from Jason’s recent article in Cleanroom Technology. Read Part 1 here.
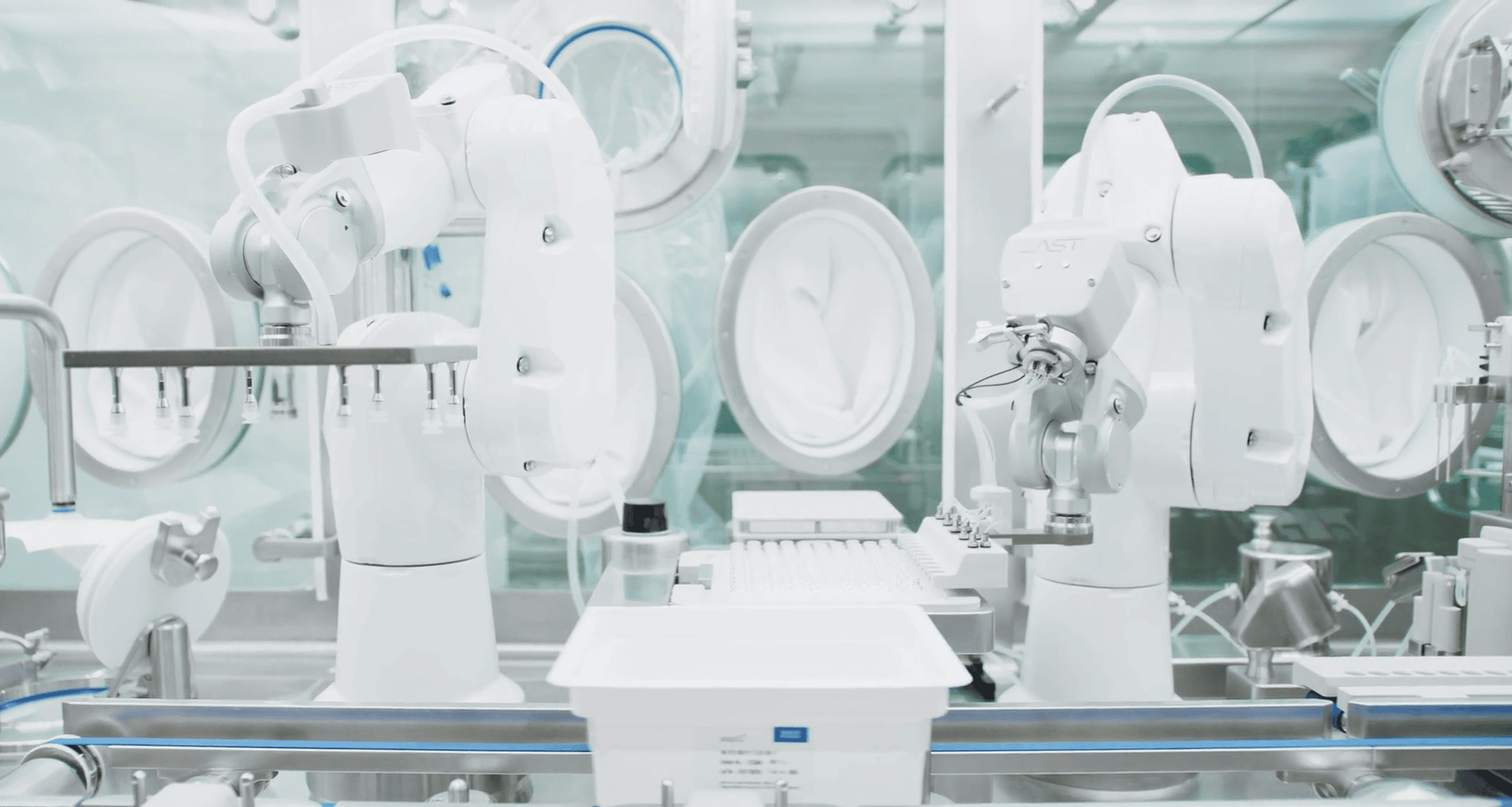
ATMPs like cell and gene therapies (CGTs) represent an exciting avenue for product development across pharmaceutical manufacturing and have led to breakthroughs in patient-centered medicine. The targeted nature of CGTs requires facilities to be designed around specific process parameters, quality-based principles, and built-in flexibility. AST’s Principal CQV Engineer, Jason Rossi, weighs in on common errors and solutions when planning operations and contingencies for production.
1. Underestimating Utilities
In cell and gene therapy manufacturing, the stakes are always high, especially for the patient. Downtime is never just downtime; it could mean a lost viability window and ultimately a lost treatment opportunity for a patient. A large part of successful cell and gene facility design is redundancy and contingency planning, and utilities are an essential part of that conversation. Do you have backup systems in place to cover all critical operations? Critical operations must be supported by appropriately classified backup systems. Are you prepared when, for example, equipment autoclaves go down for preventative maintenance? Designing in more utility capacity prevents downtime and saves on additional construction costs and re-validation.
2. Having Nothing to “Break in Case of an Emergency” – When Power Loss Becomes Product Loss
Imagine this: Crucial donor material is being processed from an immunocompromised patient who just underwent leukapheresis. The process has to be done sparingly to protect the patient, sometimes taking weeks between blood draws. The batch is midway through, and a worst-case scenario happens: the power to your facility goes out. What happens next? The question becomes whether adequate contingency power systems are in place to sustain critical operations. It’s vital to understand the needs in your facility around an uninterrupted power source (UPS) versus delayed backup power, a distinction that can often be underconsidered in contingency planning.
3. Not Considering Realistic Heat Load and Capacity Needs
Whether it’s exceeding the allotted personnel or adding equipment, once an operation’s workflow demands are in real time, there’s an understandable tendency to overuse a space. If you’re using a room beyond initial capacity estimates, high heat loads likely don’t reflect an HVAC issue; they reflect a planning issue. It can be challenging to accurately predict the exact capacity of air handling you’ll need in a room. A practical solution here is to err on the side of caution and design rooms to a grade above what they’ll be running at in practice. This accounts for possible expanded growth and provides manufacturers with an additional layer of flexibility.
4. Not Accounting for The Full Equipment Lifecycle During Installation and Integration
Every manufacturing operation, especially those producing cell and gene therapy products, understands the value of reducing downtime. Three aspects of equipment integration should always be considered in this equation: initial installation and logistics, service needs, and the preventative maintenance program. A biosafety cabinet comes with fewer limitations than larger equipment like isolators or, larger still, bioreactors. Service access planning for installation, clearance, maintenance, and calibration should all be detailed in the facility design.
5. Following Drug Substance Principles Instead of Drug Product Principles
Much of the risk in misapplying traditional pharmaceutical standards to cell and gene therapies arises from adhering to drug substance standards rather than drug product standards. The latter is considered a non-sterile process in design and is subject to additional formulation and filtration. This isn’t the case in cell and gene manufacturing, where, in many instances, the final drug product and drug substance are nearly identical. What does this error practically look like in the cleanroom? Mis-graded operations, improper pressure cascade design, and skip-grade setups are aspects that can be easily improved by adopting a more principled aseptic processing approach.
To explore how Jason and his team can support your CQV and GMP project needs, check out AST’s aseptic processing and CQV training and services available from AST Academy.